Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
23.1 Introduction
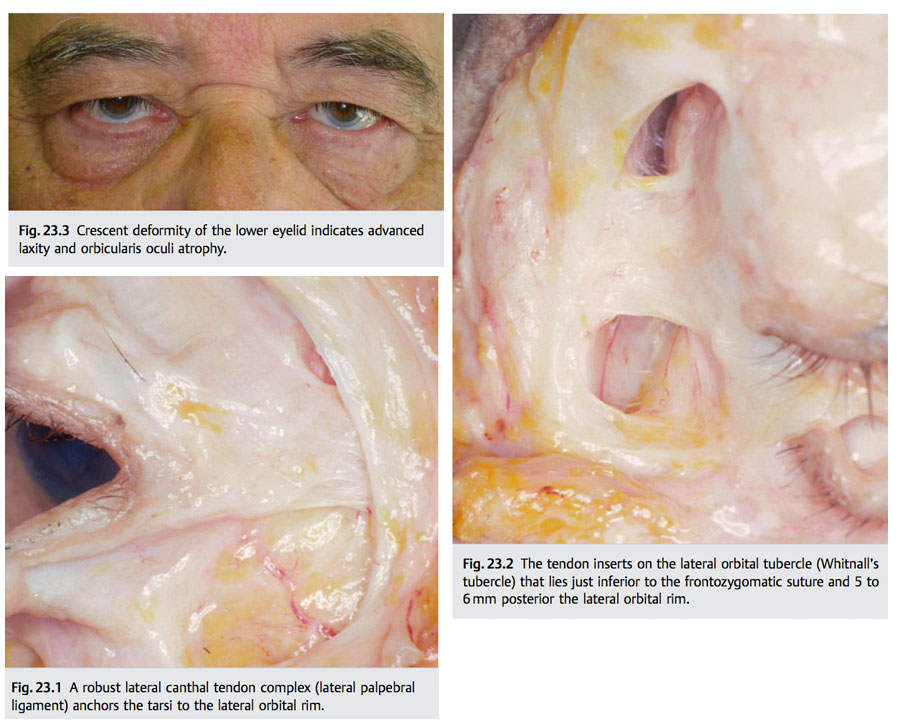
The lateral canthus is an important aesthetic facial landmark. It is formed by fusion of the upper and lower tarsal plates and is supported by muscular and fibrous lateral orbital attachments (▶ Fig. 23.1). The posterior limb of the canthal tendon (lateral palpebral ligament) anchors the tarsi to the internal zygoma at the lateral orbital tubercle (Whitnall’s tubercle) (▶ Fig. 23.2). The comparatively diminutive anterior limb interdigitates with the orbicularis oculi muscle. In addition to supporting the lower eyelid, it limits medial displacement of the tarsi during blinking. Age-related attenuation of the canthal constituents, particularly the tarsoligamentous, imparts laxity to the lower eyelid. Unrecognized or untreated lower lid laxity may contribute to well-recognized deformities after aesthetic eyelid surgery, such as the round-eye syndrome, canthal malposition, and scleral show. Functional consequences may also result if eyelid blink and tear drainage are compromised. An extensive literature describes these multifaceted problems and viewpoints regarding their diagnosis and treatment.1,2,3,4,5,6,7,8 This chapter describes the prevention or reconstruction of these complications.
23.2 Lateral Canthal Morphology
The lateral canthus is typically higher than the medial; thus, the lid ascends over its course from the medial to lateral osseous attachment. Exceptions occur, however, and comparison of photographs from a younger age with preoperative pictures is valuable in assessing age-related or postoperative position changes.
23.3 Lid Laxity: Evaluation
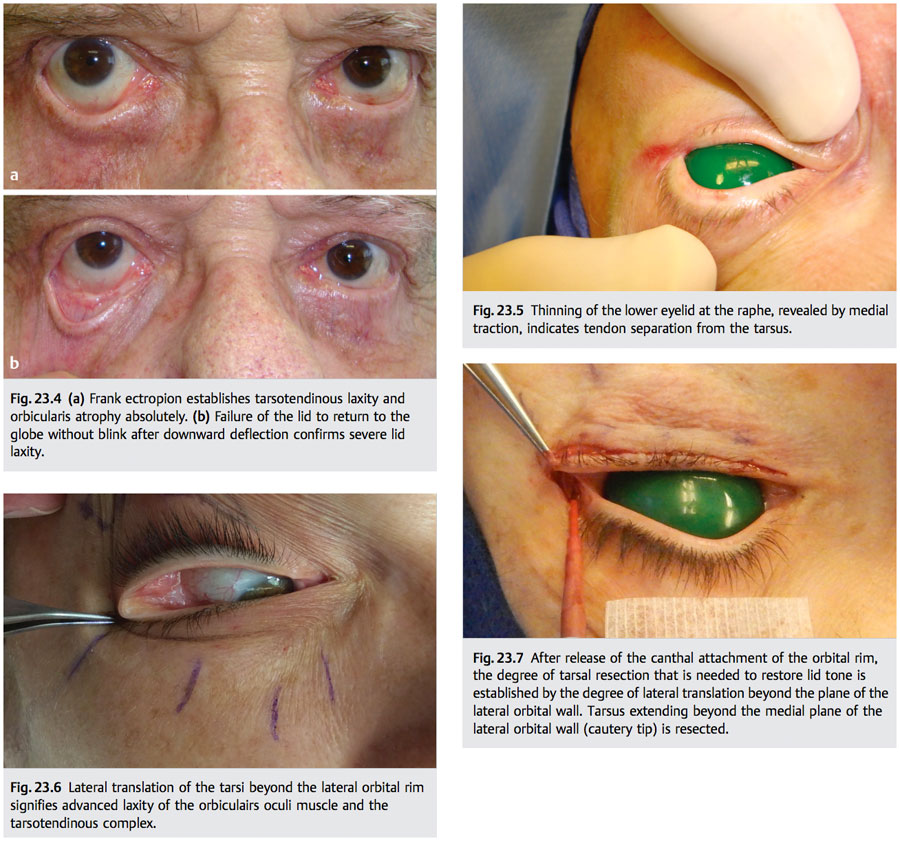
Lower eyelid shape and appearance at the canthal angle are important indicators of orbicularis oculi muscle tone and tarsotendinous status. A crescent-shaped lower lid contour or lower lid descent at the lateral limbic line implies anterior lamella laxity, possible orbicularis atrophy, and tendon dehiscence (▶ Fig. 23.3). Frank ectropion (▶ Fig. 23.4a) or failure of the lid to return to the globe after downward displacement (without blinking) establishes advanced laxity of both muscular and eyelid ligamentous elements (▶ Fig. 23.4b). Horizontal fissure effacement (i.e., phimosis) and widening of the lateral canthal angle indicate tarsotendinous separation at the lateral orbital rim.
The foregoing changes in lid and canthal morphology alert the surgeon to eyelid laxity during preoperative examination. Intraoperative evaluation definitively refines its cause and degree. Thinning of the lower lid margin at the raphe indicates tarsal distraction from the tendon (▶ Fig. 23.5). If the lateral eyelid can be displaced no farther than the plane of the medial aspect of the lateral rim, tarsal laxity is mild. Eyelid translation beyond this plane indicates moderate to severe loss of tension and mandates tarsotendinous reconstruction and orbicularis tightening, as discussed in the following
section (▶ Fig. 23.6).
23.4 Lid Laxity: Treatment
Numerous techniques restore tarsotendinous tension. Bick’s tarsal resection improves eyelid tension and does not disrupt the canthus.8,9 Shortening of horizontal fissure length and increased tension on tendon attachment to the tarsus, with the attendant risk of recurrent laxity, are disadvantages.
The tarsal strip technique re-creates a neocanthal tendon from the terminal lower tarsus.10 It is effective and avoids Bick’s disadvantages but may misalign the upper and lower eyelids. Alternatively, direct reapproximation of both the terminal upper and lower tarsi to the periosteum at Whitnall’s tubercle restores tension while preserving the eyelid’s lateral anatomical relationships (see later). It also permits vertical modification of canthal position relative to the medial canthus.
Mild laxity requires only suture fixation of the tarsi to the periosteum at Whitnall’s tubercle, as discussed later herein.
Moderate to severe laxity is treated by tarsal resection. The amount of tarsal resection required is assessed by the lateral translation maneuver: the osseous attachments of lower tarsus (posterior canthal tendon, capsulopalpebral fascia, orbital septum) are first released from the canthal tendon, and the tarsus is drawn laterally with moderate tension. Tarsus extending beyond the plane of the medial aspect of the lateral orbital wall is resected (▶ Fig. 23.7).
To re-create the tarsoperiosteal attachment, a double-armed 5–0 nylon (Ethicon S-22) (preferred) or 4–0 Polydek (Deknatel ME-2) enters the terminal tarsus of the lower eyelid and then the upper eyelid (▶ Fig. 23.8). The needles consecutively purchase the soft tissue overlying the lateral tubercle on the correct vertical plane (typically slightly higher than the medial canthal tendon) (▶ Fig. 23.9). From this coordinate, they scythe anteriorly along the orbital wall periosteum, exiting the soft tissue at the orbital margin (▶ Fig. 23.10a).
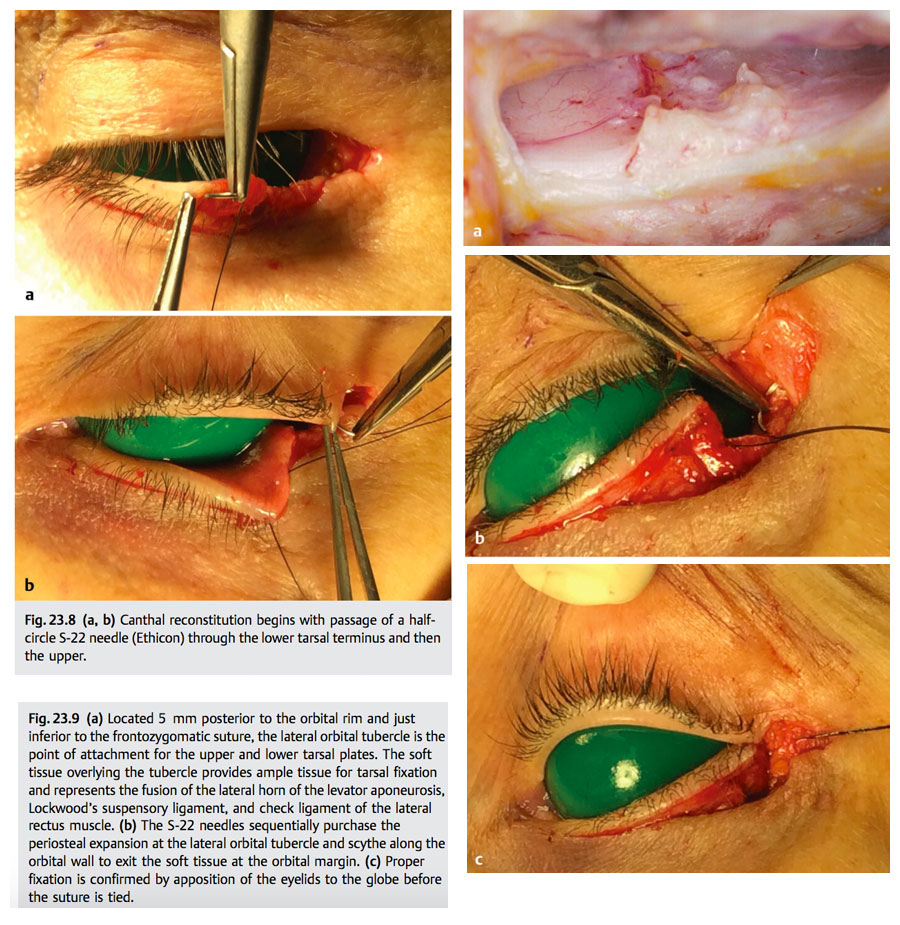
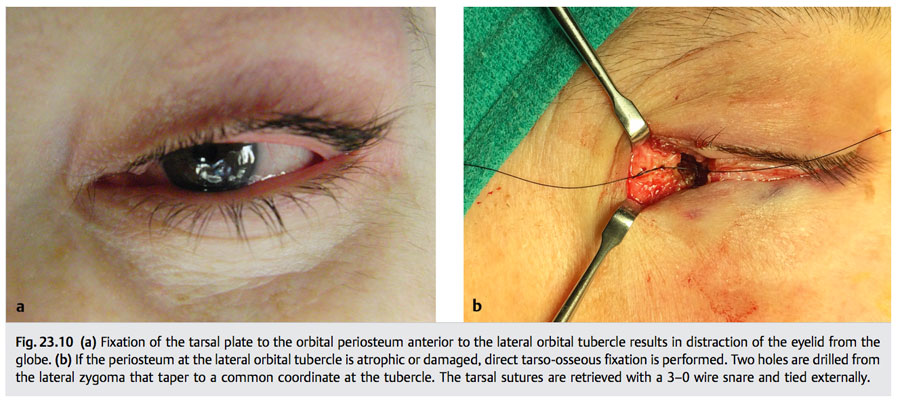
Positioning the fixation suture at the lateral orbital tubercle ensures correct eyelid contact with the globe. Although tissue is usually adequate for suture fixation at this point, periosteal degloving or atrophy may prevent secure fixation. In this case, the tarsi are anchored by drilling two holes in the lateral orbital wall that converge to Whitnall’s tubercle. The tarsal sutures are retrieved with a 3–0 wire snare and tied at the lateral rim (▶ Fig. 23.10b).
23.5 Postoperative Canthal Syndromes: Surgical Management
Accurate analysis of the cause or causes of postblepharoplasty canthal and eyelid malposition is essential to successful repair.
23.5.1 Anterior Tarsal Malposition
Uncorrected tarsotendinous laxity and incorrect tarsoperiosteal attachment to the orbital rim explain most canthal malpositions. Fixation of the tarsus or tarsi to the anterior orbital rim produces separation between the eyelids and globe (▶ Fig. 23.10). This condition may be purely aesthetic, or it may produce epiphora, ocular dryness, or both. It is caused by anterior suture fixation or inadequate periosteal support. If the periosteum is robust, refixation of the tarsi to the periosteum of the lateral tubercle is curative. If inadequate, transzygoma suture fixation is used. Orbicularis suspension further supports the canthus and firms the lower eyelid (▶ Fig. 23.11).11
23.5.2 Scleral Show and Canthal Dystopia
Excess skin resection, postoperative cicatricial lid retraction, and unrecognized negative vector (high myopia, exophthalmos, and malar hypoplasia) are factors that may complicate canthal malposition correction. Failure to neutralize vertical traction on the lid and canthus is tantamount to failure in the restoration of canthal architecture, as lid tightening alone will not mitigate vertical vectors. In cases of cicatricial lid retraction, with or without skin overresection, downward traction on the lid and canthus increases during the first 6 to 8 postoperative weeks. Corrective measures during this period typically fail. In severe cases, up to 12 months may elapse before normal viscoelastic properties return. Reconstruction is undertaken when the wound-healing continuum favors a successful outcome. To this end, eyelid pliability and vertical mobility are assessed at monthly intervals, beginning at the first postoperative visit. Evaluation continues until it is clear that the improvement trend has ended. The objective of this observation period is to allow time for the deformity to resolve, as many do, and, failing resolution, to permit application of the most aesthetically acceptable reconstructive formulation. Mild and moderate scleral show with canthal displacement with mild skin overresection, after incision maturation, is initially corrected by tarsoperiosteal fixation supplemented by orbicularis oculi muscle suspension (▶ Fig. 23.12). This method is rarely effective in severe scleral show. The distinction between a moderate and severe deformity, however, is a matter of experience and is not easily drawn. Advanced cases typically require anterior lamellar lengthening, but skin grafting is rarely an acceptable aesthetic option unless sufficient donor eyelid skin is available. Supraclavicular split-thickness grafts approximate eyelid thickness and color. Retroauricular and preauricular skin is generally too thick for eyelid application. Subperiosteal midfacelift, executed through a canthofornix exposure with orbitozygomatic and orbitomaxillary fixation, may relieve vertical traction sufficiently to obviate skin grafting. This method additionally offers improved aesthetic outcomes (▶ Fig. 23.13). With advanced skin shortage, however, canthal position improvement may not be accompanied by equivalent resolution of scleral show (▶ Fig. 23.14).
23.6 Discussion
Preoperative identification of risk factors for lower lid and lateral canthal complications, lid laxity in particular, is essential to achieving refined outcomes in aesthetic lower eyelid surgery. Lower lid tone is evaluated preoperatively and intraoperatively to assess the need for tightening and by what method (tarsoperiosteal fixation with or without tarsal resection or orbicularis suspension). Correct management of lateral canthal components essential to restoration of lid tone is straightforward. Joining the upper and the lower tarsus by suture before performing periosteal attachment minimizes common complications that occur with other methods. Positioning the lateral eyelid attachment at the lateral orbital tubercle maintains anatomical contact between the eyelids and the globe.

Intraoperative prevention of canthal and lid complications of lower blepharoplasty, in addition to lid tightening, depends heavily on minimizing vertical and horizontal forces of wound contracture. Avoiding overresection of skin during lower blepharoplasty is of utmost importance. There is, however, no unerring method for determining skin excess in the lower eyelid. Preoperatively, the pinch technique provides an estimate, but it may lead to overresection unless the lower lid is in its anatomical position as the test is performed (▶ Fig. 23.15). This method does not consider risk factors such as patient age, orbicularis atrophy, ligamentous atrophy, negative vector, or dry-eye symptoms, all of which influence the degree of skin removal. Intraoperative pitfalls that are inherent include overstretching of skin during redraping and unrecognized inferior lid margin displacement during skin resection (▶ Fig. 23.16). The latter may lead to significant skin overresection. Both are avoided by maintaining the eyelid’s anatomical position by traction suture during measurement and resection (▶ Fig. 23.17). Further, draping the skin superiorly without medial or horizontal traction further minimizes risk of overresection. Abnormal projection of the globe beyond the orbital rim (e.g., high myopia, exophthalmos, malar hypoplasia) significantly increases the risk of scleral show. Thus, skin resection is conservative in this setting and follows the preceding guidance. Excessive horizontal eyelid tightening may exacerbate or create scleral show in such cases. In the presence of dry-eye symptoms or advanced age, conservative or no skin resection is advisable. Finally, consideration of adjunctive techniques that reduce the need for skin resection, such as fat repositioning, midfacelift, and orbicularis suspension is recommended during preoperative assessment.12,13,14,15 These measures tend to minimize the foregoing complications while achieving more natural outcomes.

23.6.1 Acknowledgments
The author acknowledges the valuable contribution of Kathie J. Wolford, RN, in the research and preparation of this chapter.
References
[1] McCord CD Jr, Shore JW. Avoidance of complications in lower lid blepharoplasty. Ophthalmology 1983; 90: 1039–1046 [2] McCord CD Jr, Ellis DS. The correction of lower lid malposition following lower lid blepharoplasty. Plast Reconstr Surg 1993; 92: 1068–1072 [3] Flowers RS. Canthopexy as a routine blepharoplasty component. Clin Plast Surg 1993; 20: 351–365 [4] Jelks GW, Glat PM, Jelks EB, Longaker MT. The inferior retinacular lateral anthoplasty: a new technique. Plast Reconstr Surg 1997; 100: 1262–1275 [5] Weber PJ, Popp JC, Wulc AE. Refinements of the tarsal strip procedure. Ophthalmic Surg 1991; 22: 687–691 [6] Maffi TR, Chang S, Friedland JA. Traditional lower blepharoplasty: is additional support necessary? A 30 year review. Plast Reconstr Surg 2011; 128:265–273 [7] Patipa M. The evaluation and management of lower eyelid retraction following cosmetic surgery. Plast Reconstr Surg 2000; 106: 438–459 [8] Hester TR Jr. The trans-blepharoplasty approach to lower lid and midfacial rejuvenation revisited: the role and technique of canthoplasty. Aesthet Surg J 1998; 18: 372–376 [9] Bick MW. Surgical management of orbital tarsal disparity. Arch Opthalmol 1979; 97: 2192–2196 [10] Hurwitz JJ, Mishkin SK, Rodgers KJ. Modification of Bick’s procedure for treatment of eyelid laxity. Can J Ophthalmol 1987; 22: 262–265 [11] Anderson RL, Gordy DD. The tarsal strip procedure. Arch Ophthalmol 1979; 97: 2192–2196 [12] McCord CD Jr, Codner MA, Hester TR. Redraping the inferior orbicularis arc. Plast Reconstr Surg 1998; 102: 2471–2479 [13] Hamra ST. The role of the septal reset in creating a youthful eyelid-cheek complex in facial rejuvenation. Plast Reconstr Surg 2004; 113: 2124–2144 [14] Hamra ST. The zygorbicular dissection in composite rhytidectomy: an ideal midface plane. Plast Reconstr Surg 1998; 102: 1646–1657 [15] Hester TR, Codner MA, McCord CD. The “centrofacial” approach for correction of facial ageing using the transblepharoplasty subperiosteal cheek lift. Aesthet Surg J 1996; 16: 51–58
Click here to download or print this article by Dr. Gossman.